Dr. Ka Yu TseMBBS, MMedSc, FHKAM (O&G), Cert RCOG (GONC), FRCOG
Dr. Karen Kar Loen Chan
Dr. Karen Kar Loen ChanMBBChir, FHKAM (O&G), Cert RCOG (GONC), FRCOG
MBBChir, FHKAM (O&G), Cert RCOG (GONC), FRCOG
Dr. Karen Kar Loen ChanMBBChir, FHKAM (O&G), Cert RCOG (GONC), FRCOG
Dr. Ka Yu TseMBBS, MMedSc, FHKAM (O&G), Cert RCOG (GONC), FRCOG
Dr. Karen Kar Loen ChanMBBChir, FHKAM (O&G), Cert RCOG (GONC), FRCOG
INTRODUCTION
Ovarian cancer is the eighth most common cancer among women globally,1 and it is a leading cause of death from gynaecological cancers in developed countries. With vague symptoms and lack of an appropriate screening strategy, most epithelial ovarian cancers (EOCs) are diagnosed at a late stage, and more than half of patients with advanced disease recur in the first few years. Surgery followed by adjuvant chemotherapy remains the mainstay treatment. In recent years, there are new trends in the approach to surgery, particularly in advanced disease. Meanwhile, evidence on the use of targeted therapy has emerged. Recent advances in primary treatment of ovarian cancer will be discussed in this review.
PRIMARY SURGERY
EOC is staged according to the International Federation of Gynecology and Obstetrics (FIGO) 2014 staging system. For those who are suspected to have ovarian cancer, imaging, such as computerized tomography (CT), magnetic resonance imaging (MRI), or positron emission tomography (PET) with CT or MRI, is an integral part of the work-up procedures.
Early disease
Patients with apparent early disease would undergo a staging procedure which includes a total hysterectomy, bilateral salpingo-oophorectomy, omentectomy, bilateral pelvic lymphadenectomy, and para-aortic lymphadenectomy to the level of the renal vein and peritoneal biopsies. Approximately 10–30% of patients with apparent stage 1 disease had lymph node involvement, 6% had both positive pelvic and para-aortic nodes, and 11% had para-aortic node involvement alone. The most frequent site for para-aortic lymph node involvement (for all stages) was in the left para-aortic chain above the inferior mesenteric artery.2 For mucinous carcinoma (expansile), the chance of lymph node metastases is low and systematic lymphadenectomy as part of the staging procedure may not be necessary.3–5 The standard approach is via a laparotomy with the rationale that there is less chance of rupturing the ovarian tumour and hence upstaging the disease. A midline incision is necessary to access the upper abdomen for proper assessment for disease extent. An intraoperative frozen section can help to confirm malignancy before proceeding to a full staging procedure. For patients who had an incidental finding of ovarian carcinoma by ovarian cystectomy or oophorectomy, a second operation for re-staging would be considered, especially in situations where the nodal status would alter management. In this case, as the tumour has already been removed, a laparoscopic approach may be acceptable. For women who wish to retain fertility potential, fertility-sparing surgery with preservation of the other ovary and the uterus may be considered for serous, endometrioid, or mucinous expansile subtypes confined to one ovary (stage 1A). For those who have stage 1C1 disease, fertility-sparing surgery may still be acceptable as most recurrences are in the contralateral ovary, amenable to salvage surgery. However, for those with stage 1C2 or above or high-grade disease, fertility-sparing surgery is not advised.5 Conservative procedure should only be considered after an appropriate staging procedure.
Late disease
For those who have suspected advanced disease clinically or radiologically, the management is individualized. Treatment usually involves surgery followed by chemotherapy. The aim of surgery is to debulk all the disease completely, but clinicians need to balance the likelihood of optimal debulking and surgical morbidity.
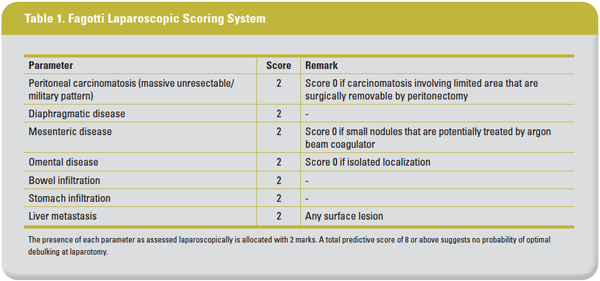
The extent of disease should be carefully assessed preoperatively to determine if optimal debulking can be achieved. Optimal debulking, defined as residual disease of <1 cm (R1) or even no gross macroscopic residual disease (R0), could provide a survival benefit. Bristow, et al, showed that each 10% increase in the maximal cytoreduction would result in a 5.5% increase in the median survival.6 Chang, et al, also demonstrated that each 10% increase in the proportion of patients having R0 or R1 could lead to an increase in median survival of 2.3 and 1.8 months, respectively.7 In order to achieve R0, it is not uncommon that radical cytoreduction is required, including diaphragmatic stripping/resection, liver resection, splenectomy, pancreatectomy, porta hepatis dissection, bowel resection, and so on. In a retrospective review including 620 patients, 138 (22.3%) developed grade ≥3 complications and 55 (8.9%) patients died within 90 days of surgery.8 With the potential surgical complications, primary debulking surgery (PDS) might not benefit those with extensive disease where optimal debulking is not feasible. Various methods were developed to select the candidates for PDS. Among all patients, the most commonly used is laparoscopic assessment using the Fagotti’s score. Using seven parameters (see Table 1), the overall accuracy rate ranged between 77.3–100% and this system has been externally validated.9
The role of routine lymphadenectomy in PDS for advanced disease is controversial. A previous randomized trial showed that systematic lymph node dissection (LND) improved the 5-year progression-free survival (PFS) rate (31.2% vs 21.6%) and median PFS (29.4 vs 22.4 months), but not the 5-year overall survival (OS) rate (48.5% vs 47%) compared with those who had resection of bulky nodes only.10 However, the recent Lymphadenectomy in Ovarian Neoplasm (LION) study, which consisted of over 600 patients with stage IIB–IV diseases who had normal lymph nodes, both before and during surgery and had no gross residual disease at PDS, were randomized to either LND or no LND.11 Both LND or no LND groups showed no difference in median OS (65.6 vs 69.2 months; hazard ratio [HR], 1.06, 90% CI, 0.83–1.34; p=0.65) and median PFS (25.5 months for both groups; HR, 1.11, 90% CI, 0.92–1.34; p=0.29), but more surgical complications were observed, including death within 60 days after PDS (3.1% vs 0.9%; p=0.049). Therefore, it is acceptable to only debulk enlarged lymph nodes instead of performing a systematic dissection in advanced disease.
NEOADJUVANT CHEMOTHERAPY FOLLOWED BY INTERVAL DEBULKING SURGERY
PDS can reduce the tumour load in a short time and may avoid the emergence of chemo-resistance. However, patients with extensive disease where optimal debulking is not feasible, or those with poor health condition like massive pulmonary embolism or extreme malnutrition, neoadjuvant chemotherapy (NACT) followed by interval debulking surgery (IDS) is another treatment option. Two similar trials, the European Organisation for Research and Treatment of Cancer (EORTC) 55971 trial and CHORUS trial, demonstrated that patients with advanced EOC receiving NACT followed by IDS and further chemotherapy did not have a worse prognosis compared with those receiving PDS followed by adjuvant chemotherapy.12–13 Patients in the NACT arm also had a lower incidence of surgical morbidity compared with the PDS arm. The Italian SCORPION trial also showed that NACT was associated with less grade 3 or 4 perioperative major morbidity (52.7% vs 5.7%; p=0.0001) and better quality of life, such as emotional and cognitive functioning, than those receiving PDS. Nevertheless, some criticized that the surgical skills were not standardized, and there was uneven distribution of the patient characteristics in both arms of these trials.
IDS is usually performed after 3–4 cycles of NACT when the tumour load has reduced and optimal debulking becomes feasible, or when the patients’ condition improve. The drop in CA 125 level and the resolution of clinical ascites might predict complete cytoreduction.14 There was no prospective trial to evaluate the role of routine LND during IDS. Apart from one Korean retrospective study that showed a better PFS and OS with systematic LND (lymph node count ≥20) vs lymph node sampling (lymph node count <20),15 no other studies have demonstrated a therapeutic value of routine systematic LND.16–17
HYPERTHERMIC INTRAPERITONEAL CHEMOTHERAPY
Hyperthermic intraperitoneal chemotherapy (HIPEC) is a new form of treatment used together with cytoreductive surgery that delivers heated chemotherapy intraoperatively after optimal debulking. With this treatment, chemotherapy can be dispersed to all areas inside the peritoneal cavity and be directly absorbed by the tumour cells. The hyperthermia can also induce thermal cellular damage, increase DNA crosslinking, and increase drug penetration into tumour cells, thus enhancing the cytotoxicity of the chemotherapy to both platinum-sensitive and resistant cell lines.18
A previous meta-analysis showed that cytoreduction and HIPEC followed by intravenous chemotherapy could result in a significantly better OS than cytoreduction and chemotherapy alone. The benefit could last for up to 8 years in the primary setting and up to 3 years in the recurrence setting.19
In a phase III, randomized trial of stage III patients who had NACT, researchers found that there was an improvement in PFS (14.2 vs 10.7 months; p=0.003) and OS (45.7 vs 33.9 months; p=0.02) for those who received HIPEC compared with the control group at the time of IDS after NACT.20 However, there was an imbalanced in the distribution of patients with unfavourable cell types between two groups. Furthermore, the selection criteria for undergoing NACT or PDS were not stated, and the study was not stratified by important prognosticators (eg, BRCA status and histological type).21 In contrast to another trial by Lim, et al, the preliminary result did not show any benefit from HIPEC at IDS, though they included stage IV patients in this trial.22 Therefore, HIPEC is still not regarded as a standard treatment.5
ADJUVANT CHEMOTHERAPY – DOSE-DENSE CHEMOTHERAPY
Most patients diagnosed with ovarian cancer will receive adjuvant chemotherapy post-surgery, which can significantly prolong PFS and OS.23 However, given its non-apparent benefits in some early-stage subtypes, adjuvant chemotherapy may be omitted for grade 1–2 stage 1A endometrioid and mucinous (expansile invasion) and stage 1A low-grade serous carcinoma. In addition, the benefit is uncertain for stage 1A-1C1 clear-cell carcinoma, stage 1B-C grade 1–2 endometrioid, stage 1C grade 1–2 mucinous (expansile invasion), and stage 1A mucinous (infiltrative invasion) tumours, and the decision for adjuvant chemotherapy should be made individually.5
Platinum-based chemotherapy remains the first-line chemotherapy in EOC. The most common regimen is 3-weekly carboplatin and paclitaxel for six cycles after primary surgery. The Japanese Gynecologic Oncology Group 3016 study showed that dose-dense chemotherapy, ie, 3-weekly carboplatin (area under the curve [AUC]=6) and weekly paclitaxel (80 mg/m2 on day 1, 8, and 15) could lead to a better PFS (28.2 vs 17.5 months; p=0.0037) and OS (100.5 vs 62.2 months; p=0.039) in stage II–IV EOC compared with the conventional 3-weekly regimen.24
In the MITO-7 trial, there was no PFS difference between the conventional 3-weekly regimen vs weekly carboplatin (AUC=2) and paclitaxel (60 mg/m2).25 However, the weekly regimen was associated with a lower incidence of grade 3–4 neutropenia, neutropenic fever, grade 3–4 thrombocytopenia, and grade ≥2 neuropathy than the conventional 3-weekly regimen.
The GOG-0262 study compared the dose-dense vs the conventional regimen with or without concomitant bevacizumab. Among women who were not receiving bevacizumab, the dose-dense regimen led to a longer PFS than the conventional regimen (14.2 vs 10.3 months; p=0.03).26
The recently published ICON-8 study consisted of over 1,500 stage IC–IV patients who were randomized to receive 3-weekly carboplatin (AUC=5 or 6) and paclitaxel (group 1), 3-weekly carboplatin and weekly paclitaxel (group 2), or weekly carboplatin and paclitaxel (group 3). Results showed that there was no difference in the restricted mean survival time or median PFS among the three groups.27 There were more grade 3/4 adverse events in the weekly groups compared with the 3-weekly groups (group 1: 42%, group 2: 62%, and group 3: 53%), which were mostly to uncomplicated neutropenic fever, which may be potentially related to the weekly full blood count test. The OS result was not yet available.
TARGETED THERAPY
Bevacizumab
Bevacizumab (Avastin) was the first approved targeted drug for ovarian cancer. It is a recombinant humanized monoclonal IgG1 antibody targeting vascular endothelial growth factor (VEGF)-A. Bevacizumab can inhibit neovascularization and modify the structure of the blood vessels. The GOG 218 study randomized suboptimally debulked stage III or IV patients to receive standard chemotherapy comprising IV carboplatin and paclitaxel, chemotherapy with concurrent bevacizumab (15 mg/kg) at 2nd-6th cycles, or chemotherapy with concurrent bevacizumab, and then 16 cycles of bevacizumab as maintenance. Results demonstrated a significant improvement in median PFS in favour of the third regimen (10.3, 11.2, and 14.1 months, respectively; HR, 0.717, 95% confidence interval [CI], 0.625–0.824; p<0.001).28 The ICON 7 study comparing chemotherapy with or without concurrent bevacizumab (7.5 mg/kg for up to 12 cycles ) in patients with stage IIb–IV disease showed similar results. Patients with suboptimally debulked stage III or IV disease who received bevacizumab had a better PFS (18.1 vs 14.5 months; p=0.04) compared with the chemotherapy alone group.29 At a follow-up analysis of 48.9 months, the high-risk group (stage III or IV who were inoperable or had suboptimal debulking) had an improved restricted mean PFS (20.0 vs 15.9 months; p=0.001) and restricted mean OS (39.3 vs 34.5 months; p=0.03) compared with the non-high risk group.30–31 The main side effects included hypertension, proteinuria, delayed wound healing, fistula, and bowel perforation, as well as a small risk of thromboembolic events.
The French, phase II, ANTHALYA trial showed that in the neoadjuvant setting, the addition of bevacizumab to a chemotherapy regimen comprising carboplatin and paclitaxel could lead to a higher complete resection rate at IDS vs chemotherapy alone (58.6% vs 51.4%).32 The incidence of grade ≥3 adverse events in both groups were similar and were mainly haematological, lymphatic, gastrointestinal, and postoperative, including wound and infectious complications.
In the phase IV, MITO16A-Mango OV2A trial, the unplanned analysis showed that among 79 patients who received NACT with bevacizumab followed by IDS, 63.5% had R0 after IDS, 86.5% were optimally debulking (residual disease ≤1 cm), and only 13.5% were suboptimally debulked (residual disease >1 cm).29
Poly (ADP-ribose) polymerase inhibitor
About 50% of EOC have defective DNA repair via homologous recombination. Under normal circumstances, single-strand DNA breaks (SSBs) can be repaired by poly (ADP-ribose) polymerase (PARP). Inhibiting PARP can cause an accumulation of DNA damage leading to double-strand DNA breaks (DSBs). Homologous recombination repair (HRR) is an essential mechanism in repairing DSB. Among patients with homologous recombination deficiency (HRD), including those who have germline/somatic BRCA mutation, PARP inhibitor (PARPi) induces synthetic lethality and hence cell death by preventing repairs of SSBs, resulting in irreparable DSBs. Recent clinical trials have demonstrated that PARPi is one of the most promising targeted agents, especially for patients with HRD.
Platinum sensitivity appears to be the strongest predictor for benefit from PARPi. There were four phase III randomized trials published in late 2018–2019 investigating the roles of PARPi in stage III-IV ovarian cancer patients after having a complete or partial response to platinum-based chemotherapy at the primary setting. The SOLO-1 study randomized patients with germline or somatic BRCA mutation to receive either olaparib or placebo, and showed that the 3-year PFS rate dropped by 70% in the olaparib group (60% vs 27%; HR, 0.30, 95% CI, 0.23–0.41; p<0.001).33 The PRIMA/ENGOT-OV26/GOG-3012 study included both HRD positive, negative, or unknown patients.34 In HRD-positive patients, median PFS in the niraparib and control groups was 21.9 and 10.4 months, respectively (HR, 0.43, 95% CI, 0.31–0.59; p<0.001). The PFS benefit of niraparib over placebo remained evident in the overall population (13.8 vs 8.2 months; HR, 0.62, 95% CI, 0.50–0.76; p<0.001). The VELIA/GOG-3005 study evaluated treatment with veliparib plus chemotherapy, and then veliparib alone as maintenance therapy.35 It was shown that there was a significant improvement in median PFS in the BRCA-mutation cohort (34.7 vs 22.0 months; HR, 0.44) and HRD cohort (31.9 vs 20.5 months; HR, 0.57), as well as the intention-to-treat population (23.5 vs 17.3 months; HR, 0.68). The GINECO/ENGOTov25 PAOLA-1 trial investigated the effects of combining PARPi with bevacizumab. Patients with advanced disease who were given carboplatin and paclitaxel with bevacizumab were randomized to receive either olaparib or placebo. The median PFS was better in the olaparib plus bevacizumab arm than the placebo arm (22.1 vs 16.6 months; HR, 0.59; p<0.001).36 The hazard ratio was 0.33 and 0.43 among HRD patients with and without somatic BRCA mutation, respectively, but no significant difference was observed in patients with HR proficient tumours. Therefore, it appeared that patients with BRCA mutation or HRD in the tumour could benefit most from PARPi. Testing for BRCA1/2 mutations has been recommended for all patients with non-mucinous ovarian cancer while testing for other HR genes mutation (such as RAD51C/D, BRIP1, PALB2) should be considered.5
CONCLUSION
Improving survival in patients with ovarian cancer remains a challenge. An optimal surgical effort is the cornerstone of a good outcome. Recently, new treatment modalities such as HIPEC and targeted therapy have emerged. Active research is underway to better delineate their effectiveness in patients with different disease status. Until now, only two targeted therapies – bevacizumab and PARPi – have been approved for ovarian cancer to date, with ongoing studies on different combinations of these agents. More research is needed to identify biomarkers that can select patients who may respond to these agents. These recent advances open up a new paradigm in ovarian cancer treatment.
About the authors
Dr Ka Yu Tse is a Clinical Associate Professor from the Department of Obstetrics & Gynaecology, The University of Hong Kong, Queen Mary Hospital, Hong Kong. Conflict of interest: None.
Dr Karen Kar Loen Chan is a Clinical Associate Professor from the Department of Obstetrics & Gynaecology, The University of Hong Kong, Queen Mary Hospital, Hong Kong. Conflict of interest: None.