Managing adult ADHD in primary care
01 Sep 2020

Attention-deficit/hyperactivity disorder (ADHD) has traditionally been perceived as a childhood condition. Audrey Abella speaks with Dr Lim Boon Leng, psychiatrist at the Centre for Psychological Wellness at Gleneagles Medical Centre, Singapore, to shed light on adult ADHD and share insights on managing this condition in primary care.
Introduction
Previously, the consensus has always been that the hyperactivity and attention deficit symptoms in children with ADHD will improve and remit as they mature neurodevelopmentally. However, in the past decade, research about adult ADHD has shown that up to 30–50 percent of children with ADHD will have significant symptoms that will persist and require treatment in adulthood. While there has been no epidemiological study on the prevalence of ADHD among adults in Singapore, a US study estimated its prevalence to be about 2.5 percent.
Despite the growing awareness in adult ADHD, many healthcare professionals are reluctant to consider the diagnosis in the clinical context. This could be due to their sustained hold on the traditional, albeit outdated, view that ADHD does not exist in adults. Another issue would be the abuse factor among individuals who seek stimulant medications for non-therapeutic purposes.
However, if left untreated, adult ADHD may lead to chronic and potentially debilitating impairments in occupational and social domains, consequently leading to adverse effects for the community at large.
For instance, untreated ADHD may hamper academic progress or work performance, and increase risk of divorce or substance abuse. Adults with untreated ADHD are more likely to be involved in road mishaps, or to be lawbreakers. As such, identifying ADHD and providing treatment are important to prevent the perpetuation of such outcomes.
At present, the pathophysiology of ADHD is not completely understood. It is believed to be a neurodevelopmental psychiatric disorder that results in attention deficits, hyperactivity, or impulsiveness deemed inappropriate for the afflicted individual’s age. Proposed mechanisms include abnormalities in functioning of neurotransmitters, brain structure, and cognitive function.
Diagnosis
Adults with ADHD can present to a GP with a myriad of concerns. They may have noticed difficulties with attention and concentration for a long time but may have put them off, assuming these are normal. They may seek help when symptoms adversely affect their work. As individuals with ADHD often have difficulties completing or even starting tasks, they are more prone to anxiety as they worry about meeting their targets. They may present to primary care with sleeplessness and psychosomatic symptoms (eg, headaches, stomach aches, muscle tension).
The gold standard in diagnosing ADHD, be it in children or adults, is a thorough clinical assessment by a mental health specialist. The Diagnostic and Statistical Manual of Mental Disorders (DSM–5) criteria for ADHD is valid for use in adults.
For a diagnosis to be made, patients ≥17 years need to have five out of the nine symptoms in either the inattention or hyperactive-impulsive symptoms criterion (Table 1) to be diagnosed with adult ADHD. Several symptoms could have been present prior to age 12. Symptoms must be present in two or more settings and there has to be clear evidence that the symptoms do interfere with, or reduce the quality of, social, academic, or occupational functioning.
Table 1: Symptoms of ADHD – The individual frequently exhibits the following:
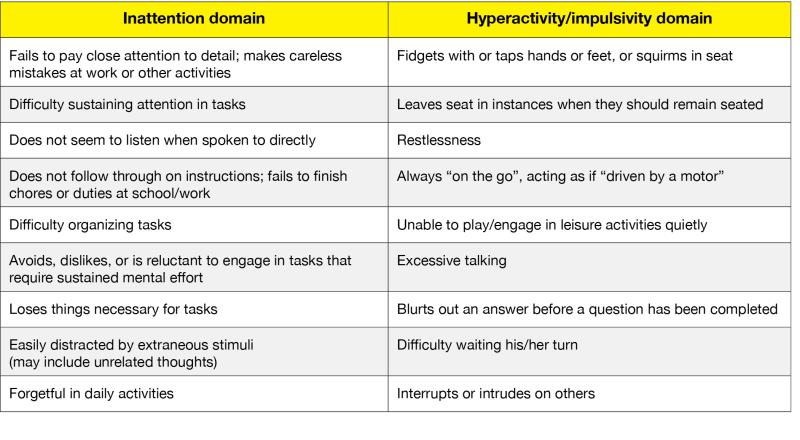
In adults, hyperactivity symptoms may often be minimal or even absent. While many adults may continue to be impulsive and fidget a little, they are often able to supress their inner restlessness and behave appropriately in social settings. The procrastination, carelessness, inattentiveness, and forgetfulness are the things that may lead to difficulties with tasks which, in turn, give them a harder time in life.
Apart from patient interviews, mental health specialists may also gather corroborative history by interviewing parents, spouses, or close friends, or examine school reports to determine the extent and validity of their patients’ symptoms. Scales and psychometric testing (eg, Conners’ adult ADHD rating scale) are widely used in some settings to assist in the diagnosis of adult ADHD. In primary care, the adult ADHD Self-Report Scale-V1.1 may be useful as an initial screening tool to help determine if specialist referral is warranted.
Clinical guidelines
Clinical guidelines for the diagnosis and treatment of ADHD are available. Locally, the AMS–MOH Clinical Practice Guidelines on Attention Deficit Hyperactivity Disorder is available online for reference.
Guidelines from the UK National Institute of Clinical Excellence (NICE) or the American Psychiatric Association (APA) are general and are not specific for adult ADHD. Both lean towards best practices in childhood ADHD. This reflects the lack of studies in adult ADHD, leading to paucity in evidence-based practice in adult ADHD.
Treatment
Adults with ADHD will most likely be referred to psychiatric specialists for confirmation of their diagnosis and further treatment. This is particularly so when stimulant medications – which are controlled substances – are required to improve their concentration and attention. Patients should be made aware that while these may improve symptoms, these are not curative.
Stimulants have the most robust evidence in the treatment of ADHD in children and adults alike, and are often recommended as the medications of choice to start off with following a diagnosis. In Singapore, only methylphenidate-based stimulants are currently available. Advantages of stimulants include their proven efficacy, fast action, and that it can be taken “as-needed”. Typically, the onset of action is ~45 minutes after consumption. Stimulants may be taken during workdays instead of daily if the patient so desires. Disadvantages however are the potential abuse and the waning therapeutic effects. Common side effects are headache, insomnia, poor appetite, and feelings of agitation.
Atomoxetine, a selective noradrenaline re-uptake inhibitor indicated for ADHD treatment, is also available locally. However, as opposed to stimulants, its therapeutic effect is gradual and subtle, and is usually apparent only after 3–4 weeks. Atomoxetine must also be taken daily to be effective. Advantages are its nonaddictive properties and a lasting therapeutic effect (24/7). Common side effects are nausea, headache, and insomnia.
Some antidepressants (eg, bupropion, amitriptyline) have been used to varying success in the treatment of ADHD and may be considered should first-line treatment fail.
Some studies have suggested that omega-3 supplementation may help in controlling ADHD symptoms. Primary care physicians may recommend omega-3 supplements as an option to patients who prefer not to be medicated due to the stigma of psychiatric treatment. Omega-3 may also be used to supplement current medications.
While medication remains the only proven way to improve concentration in ADHD patients, psychological intervention and psychotherapy may be beneficial to help patients develop coping mechanisms and strategies for managing their symptoms, and address the secondary emotional difficulties arising from their dysfunctions.
Conclusion
In conclusion, adult ADHD is often underrecognized and underdiagnosed. However, it carries with it chronic and potentially severe consequences. Effective treatment exists, which will help patients do better in work and improve their quality of life. The main role of a primary care physician in this setting is to identify the condition in individuals who present with symptoms, then advise them to seek further treatment with a specialist.
Online resources
AMS-MOH Clinical Practice Guidelines on Attention Deficit Hyperactivity Disorder
www.moh.gov.sg/hpp/doctors/guidelines/GuidelineDetails/cpgmed_adhd
Attention Deficit Hyperactivity Disorder: Diagnosis and Management
www.nice.org.uk/guidance/ng87
Diagnosis and Management of Attention-Deficit/Hyperactivity Disorder in Adults
www.aafp.org/afp/2012/0501/p890.html
Adult ADHD Self-Report Scale (ASRS-v1.1) Symptom Checklist
add.org/wp-content/uploads/2015/03/adhd-questionnaire-ASRS111.pdf
 Dr Lim Boon Leng
Dr Lim Boon Leng