Brigatinib continues to prevail in ALK+ NSCLC
30 Nov 2019
byAudrey Abella
 Dr Ross Camidge
Dr Ross CamidgeThe ALK* inhibitor brigatinib maintained its superiority over crizotinib in the treatment of ALK+ non-small-cell lung cancer (NSCLC), according to the second interim results of the ALTA-1L** trial presented at ESMO Asia 2019.
“Brigatinib represents the only once-daily, single-pill dose, next-generation ALK inhibitor with significantly superior efficacy and tolerability and better health-related quality of life (HRQoL) over crizotinib, making it a promising new first-line treatment for ALK+ NSCLC,” said Dr Ross Camidge from the University of Colorado in Aurora, Colorado, US.
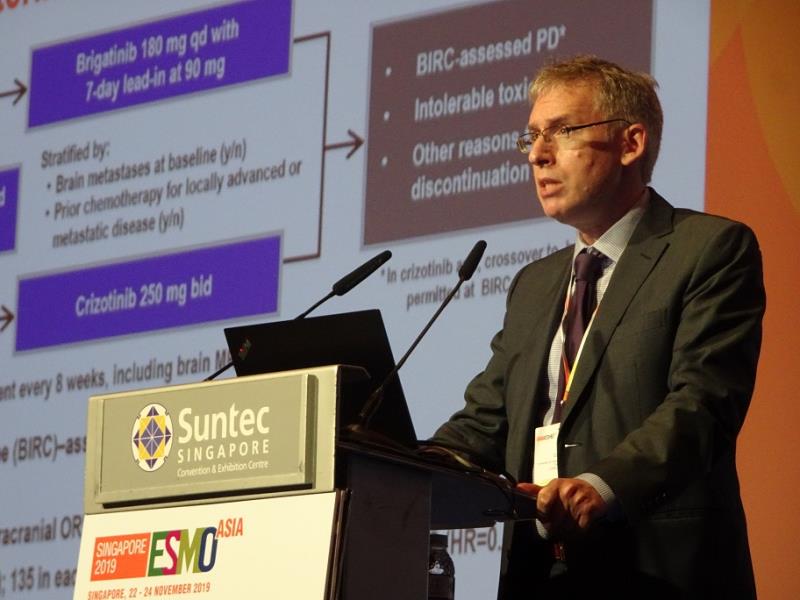
A total of 275 participants (median age 59 years, 55 percent female) were randomized 1:1 to receive either once-daily brigatinib 90 mg for a week and 180 mg thereafter or twice-daily crizotinib 250 mg. Crossover from crizotinib to brigatinib was permitted. [ESMO Asia 2019, abstract LBA1]
After a median follow-up of 24.9 months, brigatinib remained superior to crizotinib in terms of BIRC***-assessed progression-free survival (PFS; median, 24 vs 11 months; hazard ratio [HR] for disease progression or death, 0.49; p<0.001). Brigatinib also reigned across all subgroups, with the most pronounced PFS benefit in individuals with brain metastases at baseline (HR, 0.25).
The findings come on the heels of the initial interim analysis demonstrating a similar HR (0.49; p<0.001) for BIRC-assessed PFS after a median follow-up of 9–11 months, and support evidence that have consistently highlighted brigatinib as having the longest reported median PFS among next-generation ALK inhibitors#. [N Engl J Med 2018;379:2027-2039; Ann Oncol 2018;29:1409-1416; Clin Cancer Res 2018;24:2771-2779]
The CNS factor
Individuals with baseline central nervous system (CNS) metastases remained a subgroup that demonstrated the greatest differential effect between groups. Despite overlapping confidence intervals and significant benefit with brigatinib in both subgroups, those with baseline CNS disease had a consistently lower risk for disease progression or death than those without (HR, 0.25; p<0.0001 vs HR, 0.65; p=0.0298). “[Moreover,] differential progression [appeared] to be a much earlier event among those with baseline CNS disease as reflected by the earlier curve separation,” said Camidge.
The impact of baseline CNS metastases mostly comes from the dramatic worsening of PFS with crizotinib among individuals with and without CNS disease (5.6 and 13.0 months, respectively). “[This is] an effect seemingly neutralized by brigatinib, given that the median PFS in the brigatinib arm was the same [at] 24 months, regardless of the presence or absence of baseline CNS disease,” said Camidge.
OS, safety, QoL
Overall survival (OS) remains immature, with only 24 and 27 percent of the respective brigatinib and crizotinib arms having had a death event, which was consistent with the known prolonged survival in this patient population. “OS differences … are expected to be strongly confounded by the crossover built into the trial design,” Camidge pointed out. Of the 61 crizotinib recipients who crossed over to brigatinib, median BIRC-assessed PFS was 15.6 months which, according to Camidge, was highly comparable to that observed in the phase I and II trials.
Adverse events were more common with brigatinib and were dominated by laboratory abnormalities, which did not appear to be symptom-related in most cases, noted Camidge. Only 3 percent of brigatinib recipients exhibited the known rare side effect of early-onset pulmonary events, as these were mitigated/addressed with the appropriate management strategies.
Brigatinib still fared better than crizotinib in terms of HRQoL, owing to the longer median time to QoL worsening (26.7 vs 18.3 months) and duration of QoL improvement (not reached vs 12 months). “[Regarding] specific functional and symptom domains, again, no areas favoured crizotinib over brigatinib. [Although] some of the improvements favouring brigatinib could reflect greater and/or more prolonged drug efficacy, drug tolerability differences may also [factor in],” explained Camidge. “This is perhaps most clearly suggested in some of the gastrointestinal domains (eg, appetite, constipation), which favoured brigatinib over crizotinib more than five- and tenfold, respectively.”
Excellent CNS penetration
According to Camidge, the initial first-line targeted treatment paradigm for advanced ALK+ NSCLC arose from the Profile 1014 trial##, which demonstrated the significant PFS advantage of crizotinib over platinum-pemetrexed. However, the median PFS for crizotinib was only 10.9 months. “Progression on crizotinib can occur due to its known poor CNS penetration … Brigatinib [has an excellent CNS] penetration and preclinical activity against a wide range of crizotinib-resistant mutations,” said Camidge.
However, second-line data did not translate to superior outcomes, noted discussant Dr Sai-Hong Ou from the University of California Irvine School of Medicine in Orange, California, US. “[Although] brigatinib is a very potent first-line treatment option for ALK+ NSCLC with enhanced activity in the CNS … caution [is needed in] translating the second-line results to first-line efficacy.”
The effects of chemotherapy in this setting – and in brain metastases – should also be evaluated, added Ou, given its reported additive effects, to ascertain the median number of cycles necessary, response rates, and depth of response.