An Approach to Plagiocephaly in Infants and the Role of Helmet Therapy
30 Jun 2020
Dr. Pearlly Pei Qi Chang
Dr. Pearlly Pei Qi ChangMBBS, MRCPCH, M.Med (Paediatrics)
MBBS, MRCPCH, M.Med (Paediatrics)
Dr. Pearlly Pei Qi ChangMBBS, MRCPCH, M.Med (Paediatrics)
Dr. Pearlly Pei Qi ChangMBBS, MRCPCH, M.Med (Paediatrics)
INTRODUCTION
Plagiocephaly generally refers to cranial asymmetry that may arise in infants due to various reasons. The most common cause of plagiocephaly is positional plagiocephaly, also known as non-synostotic positional calvarial deformity, which may arise from intrauterine constraint or extrauterine compression. Thereafter, it may be perpetuated by post-natal sleeping position, concurrent torticollis, or other neuromuscular conditions.1
The most common form of positional plagiocephaly is posterior plagiocephaly, in which there is unilateral flattening of the parieto-occipital region resulting in a rhomboid-like shift of the calvarium with compensatory anterior shift of the ipsilateral ear, and bossing or bulging of the ipsilateral forehead. Another variant is brachycephaly, in which there is symmetrical flattening of the entire occipital region, resulting in a foreshortened anteroposterior dimension of the skull with or without an elevation of the skull vertex.1 Facial asymmetry with misalignment of the eyes and/or ears and postural congenital torticollis with restricted range of cervical and head motion may accompany the condition.2
The development and natural course of positional plagiocephaly are closely associated with the infant’s motor development in the first few months of life. In the first weeks of life, the degree of positional plagiocephaly usually worsens because the infant has little active positioning of the head. Thereafter, the head shape begins to improve in tandem with the normal course of motor development.3 The peak prevalence of positional plagiocephaly is around 4 months of age.4
The overall incidence of positional plagiocephaly has risen since the 1992 American Academy of Pediatrics (AAP) recommendation that infants should be placed on their back to sleep in order to reduce the risk of Sudden Infant Death Syndrome (SIDS).5 However, it should be taken into account that positional skull deformities such as positional plagiocephaly are generally benign. These reversible head shape anomalies mostly do not require surgical intervention, as opposed to craniosynostosis, which can result in neurologic damage and progressive craniofacial distortion. It is therefore clinically important to properly evaluate and differentiate infants with benign skull deformities from those with craniosynostosis.6 Paediatric primary care providers should be competent in diagnosing positional plagiocephaly, as keen assessment and diagnostic skills may maximize outcomes and minimize cost for families and payers through the judicious use of referrals.7
EVALUATION
A complete history, physical examination, and developmental assessment should be performed to identify any particular dysmorphic features or associated developmental delays that may suggest an underlying craniosynostosis syndrome.
Patients with positional plagiocephaly would have had a typical rounded head at birth, only developing parallelogram deformity and occipital flattening after a few weeks or months. If occipital flattening was present at the time of birth, lambdoid craniosynostosis should be considered.8
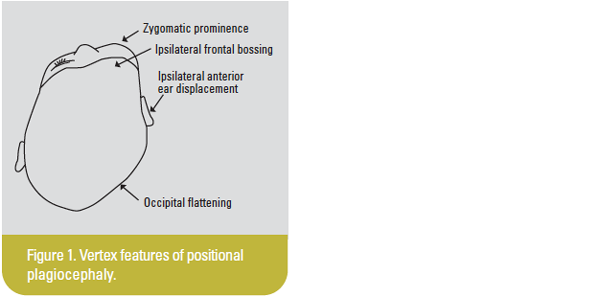
Examination of the infant’s head should include thorough observation from all angles including anterior, posterior, vertex, and lateral positions, as well as a worm’s eye view. When viewing the infant from the front, look for symmetry of the cheeks, eyes, and ears, as well as elevation of the vertex. From a posterior perspective, look for symmetry of the base of the skull as occipitomastoid bulging may indicate lambdoid craniosynostosis. From a vertex view, look for symmetry between the right and left sides by noting the relative position of the ears and zygomas. In addition to the unilateral flattening of the occipital area, there may be ipsilateral frontal and parietal bossing, zygoma prominence, and anterior ear displacement ipsilateral to the flattened occiput, forming the typically observed parallelogram (Figure 1). From the side, look for flatness on the back of the head or a high, sloping forehead, also noting the symmetry of the left and right sides. In the worm’s eye view, which may be achieved when the infant is supine, look for symmetry of the ear position, a smooth arch of the forehead, and the degree to which the cheeks are of equal height. Finally, the face should be examined for head tilt and contralateral facial flattening, neck movements assessed for any underlying torticollis, and suture lines inspected and palpated for any ridging which can indicate craniosynostosis.7–8
Three-dimensional (3D) topographical scanning may be useful for baseline assessment of severity following the diagnosis of positional plagiocephaly.9 This scan involves a light source and recorder that utilizes data obtained from the reflection of light at various angles from the infant’s head to construct a computer-generated 3D image. This procedure is often done in a clinic or practice setting and does not expose the infant to ionizing radiation.10-16 The 3D stereophotogrammetry is another similar scan which utilizes multiple camera systems to provide a 3D image.12,14,17 Although these 3D imaging techniques may provide better objectivity, such resources may not be widely available and should not be relied upon in place of clinical examination.
Most infants with positional plagiocephaly can be adequately diagnosed through detailed clinical examination alone. Only in cases wherein clinical examination is equivocal should imaging be considered to assist in the diagnosis and to exclude craniosynostosis. In such cases, a skull X-ray or an ultrasound of the suspected suture may be obtained. Although a computed tomography scan of the head is still the gold standard, rarely is it ever needed for the diagnosis of plagiocephaly or to rule out craniosynostosis. Furthermore, children, particularly infants, should be spared unnecessary radiation unless all previously performed radiological studies are truly equivocal and the benefit of making the diagnosis is deemed to be worth the radiation exposure.9 The utility of magnetic resonance imaging (MRI) for plagiocephaly has been poorly investigated18 and is therefore not recommended,9 especially considering the additional risks associated with general anaesthesia, which is usually required to facilitate an MRI scan in infants aged >3 months.
CLASSIFICATION
At present, there is no standard classification system that has been adopted to quantify and monitor positional plagiocephaly. Existing methods range from visual assessment, anthropometric measurements with a calliper or a flexicurve, plagiocephalometry (a strip of moulding thermoplastic material applied around the infant’s head at the widest transverse circumference), 3D imaging, and other radiological imaging modalities.
The ideal grading instrument should be based on clear cut-offs and repeatable measurements to ensure clinical reliability and validity, be relatively inexpensive and easy to apply within a reasonable time frame, and be easily understood by parents to allow for accurate communication between clinicians and families.
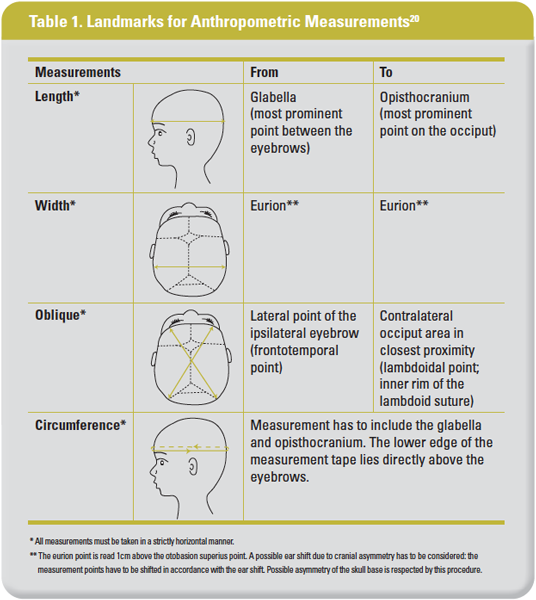
Among the existing methods, anthropometric measurements with a calliper best fulfils the requirements for an ideal grading instrument by nature of cost, availability, and ease of use, provided that measurements are taken using standardized landmarks to ensure reproducibility.19 Proposed landmarks for each of the measurements are detailed in Table 1.
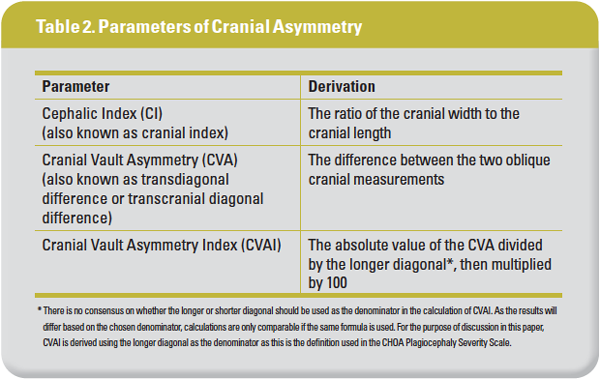
Once accurate measurements have been obtained, the parameters for cranial asymmetry can then be calculated. Common parameters used to document and quantify cranial asymmetry, such as the cephalic index (CI) and the cranial vault asymmetry index (CVAI), are defined in Table 2.
Anthropometric measurements and cranial asymmetry parameters are important to facilitate objective clinical documentation. In clinical practice, however, it is more likely that quantifiable measurements are used simultaneously with visual assessment. This is because visual assessment provides the opportunity to discuss the child’s head shape with the parents, while the quantifiable measurements allow numerical classification of the extent of asymmetry.19
The Children’s Healthcare of Atlanta (CHOA) Plagiocephaly Severity Scale21 published in 2017 was developed based on digitally obtained indices and clinical outcomes, designed with the aim of being sufficiently sensitive to detect treatment changes in infants undergoing helmet therapy. While it utilizes CVAI as the objective classification determinant, it also includes key clinical observations for each severity level, thereby acknowledging the qualitative differences that may be present to varying degrees at each level and possibly facilitating better parental understanding of the scale. This scale potentially provides a low-cost solution for measuring severity of plagiocephaly that can be easily employed in a clinical setting. However, it has yet to undergo a large-scale external validation in a prospective randomized study, particularly in a setting where the cranial measurements are obtained manually rather than digitally.
Table 3 summarizes the classification and recommended treatment according to the CHOA Plagiocephaly Severity Scale, with added illustrations of expected clinical findings.
The other most commonly referenced plagiocephaly severity scale was published by Argenta, et al, in 2004.22 As it relies solely on clinical observation, however, the interrater reliability is only moderate.19 It also does not include any quantifiable measurements, thereby making it challenging to achieve clinical objectivity.
MANAGEMENT
Prevention
Despite being benign, positional plagiocephaly and any associated craniofacial asymmetry, particularly in the more severe cases, can cause considerable anxiety among patients’ families. There is often fear or concern that the infant may have craniosynostosis. Parents may also be concerned about facial asymmetries that are noted by their family members. Certainly, for infants with severe positional plagiocephaly and craniofacial asymmetry, parental concerns about the cosmetic outcome and the potential social or psychological effects on their child are valid and very real.23 It is therefore important to educate parents from an early stage on methods to proactively decrease the likelihood of development of occipital flattening: failing which, appropriate management and referrals may be initiated as required.6
There are multiple methods to decrease the risk of developing positional plagiocephaly. Most cases can be prevented by alternating the supine head position (ie, left and right occiputs) every night during sleep beginning immediately after birth. Varying the infant’s position relative to the room entrance (where the infant’s gaze is likely to be drawn to noise and activity) also helps to avoid postural preferences in a certain direction, thus reducing the likelihood of uneven pressure on any side of the head.8 Lastly, prone positioning or “tummy time”, while the infant is awake and is being observed, will reduce the overall amount of pressure on the head. In addition, it also facilitates the development of upper shoulder girdle strength necessary for timely attainment of certain motor milestones.24
Treatment
Positional plagiocephaly is a nonoperative condition except for very rare cases.25 Modalities of treatment include observation, education on repositioning techniques, repositioning with an assistive device, physiotherapy particularly in the presence of concomitant torticollis, and helmet therapy. These may be applied individually or in combination. Principal management decisions revolve around the issue of whether conservative measures, namely observation, repositioning, physiotherapy, or combinations thereof, should be tried, how long to persist with conservative treatment prior to instituting helmet therapy, and the criteria that need to be met in order to proceed with helmet therapy.1 Reassuringly, high rates of parental satisfaction have been reported regardless of the choice of treatment modality.26
Observation
A large proportion of cases do improve over time with mere observation.27 This is in keeping with normal developmental milestones – as an infant matures, less time is spent in supine and in the same position, thus reducing pressure on the head and allowing it to reassume its former shape. Parents should be reassured that as long as the child continues to develop normally, no further intervention is usually required.
Repositioning
The aim of repositioning treatment is to reduce pressure on the affected area. Parents should be educated to incorporate repositioning techniques into the child’s routine and environment. This may include placing the infant onto their abdomen for extended periods throughout the day, repositioning the child’s head throughout the day so that the rounded side of the head is placed against the mattress, repositioning cots, and other areas that infants spend time in so that they will have to look in a different direction to see their parents or others in the room, repositioning mobiles and other toys for similar reasons, and avoiding extended time sleeping in car seats, bouncy seats, or other supine positions that might exacerbate the problem.28
There are commercially available pillows designed to assist with repositioning treatment. However, its use conflicts with the AAP’s recommendation to avoid such soft bedding items in an infant cot in order to provide a safe sleeping environment and reduce the risk of SIDS.29 Physiotherapy is therefore recommended as the preferred and safer treatment modality over repositioning with an assistive device.
Physiotherapy
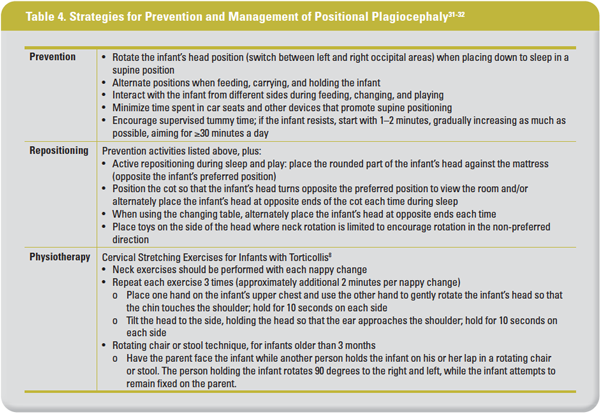
Physiotherapy is recommended over education on repositioning techniques alone, with evidence suggesting superiority particularly in cases of severe positional plagiocephaly.2 Physiotherapy interventions may include exercises to reduce positional preference and stimulate motor development,30 as well as cervical stretching exercises for torticollis. This should be done in consultation with a physiotherapist. Table 4 summarizes the main strategies for prevention, repositioning, and physiotherapy in the management of positional plagiocephaly.
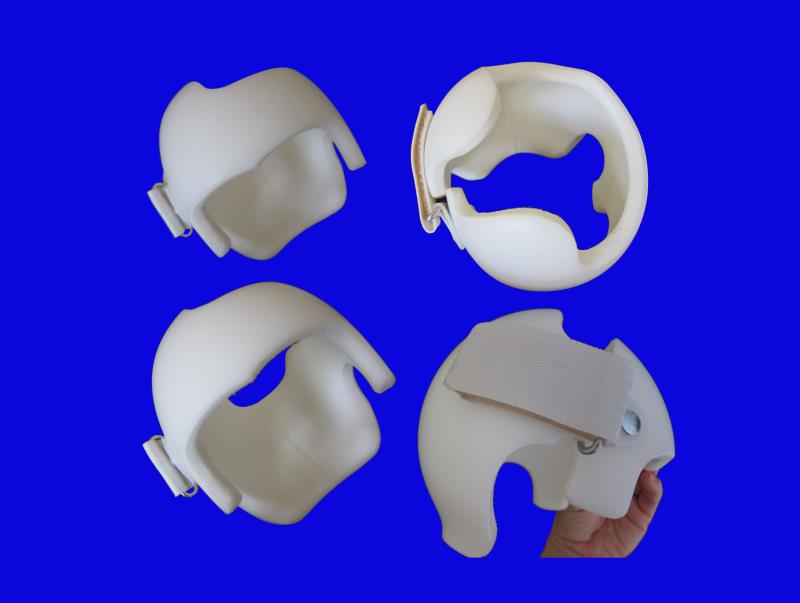
Cranial moulding orthosis therapy (helmet therapy)
Helmets are custom-fitted cranial orthoses designed to be worn 23 hours a day for several months until the child has achieved satisfactory cosmetic correction or outgrown their helmet. Frequent regular assessments are required to review cranial growth and observe for the presence of any adverse effects, as well as to make any necessary adjustments to the device to allow for continual growth and change in shape of the calvarium. These orthoses may be passive, to allow room for growth in the flattened areas, while minimal pressure is applied to the areas with bossing, or active, with compression applied to the bossed areas to achieve a more rapid deformity correction.1
The correction rate of plagiocephaly with helmet therapy decreases as the infant’s age increases. Those helmeted at ≥9 months are less likely to achieve full correction to attain normal calvarial symmetry. However, some degree of improvement may still be observed even in those commencing helmet therapy later than 12 months of age. The duration of helmet therapy also positively correlates with age. Older infants require a longer duration to achieve full correction compared with infants commencing helmet therapy at a younger age.33
The main benefit of helmet therapy is the ability to quickly achieve a treatment outcome that is equal or superior to that of repositioning in a fraction of the overall treatment time.1 Comparatively, treatment with repositioning and physiotherapy will see most cases improve by 3–5 years of age, with the majority returning to normal range, and an incidence of developmental delays no higher than what might be expected in the normal population.34
In a recently published randomized controlled trial,35 84 infants (aged 5–6 months) who previously had physiotherapy, were prospectively assigned to either helmet therapy or to “the natural course of the condition”. Blinded outcome assessment performed at 2 years of age showed no difference in change in head shape between the two groups, both with intention-to-treat and per-protocol analyses. There were also no significant differences in the secondary outcomes of parental satisfaction and anxiety, motor development, and quality of life. In addition, those who underwent helmet therapy reported one or more side effects related to it. Although this study was limited by its low participation rate, small treatment group size, lack of an objective measure of compliance to helmet therapy, differences in baseline characteristics, exclusion criteria concerns, as well an outcome subject to measurement bias,1 it nonetheless serves to illustrate that there may not be clinically meaningful differences in outcomes to strongly support helmet therapy over conservative measures.
It is therefore important to note that evidence in favour of helmet use must be tempered by the lack of data regarding the extent of natural improvement of positional plagiocephaly alongside the varying compliance rates to helmet therapy. The infant must first be amenable to wearing the helmet for the prescribed duration. Other considerations include the long-term effects of both helmet therapy vs “untreated” plagiocephaly, the costs associated with helmet therapy,1 as well as the potential complications of helmet therapy including skin reaction to helmet lining materials, skin irritation, skin breakdown and infection, pressure sores, hair loss, increased perspiration, unpleasant odour, and pain. These may result from poor observance of hygiene or from ill-fitting, poorly applied helmets.35-36 Although relatively minor, largely transient, and easily treatable, these complications remain important factors as they can directly impact patient care, comfort, and quality of life. Furthermore, the development of any side effects will affect the compliance rate, which in turn will affect the outcome.
It should therefore be emphasized to parents that although helmet therapy may result in a faster rate of improvement over a shorter period of time,1 it is not entirely risk-free, and the outcome may vary between individuals based on the degree of acceptance and compliance to therapy. The decision to proceed with helmet therapy should be carefully considered, bearing in mind that positional plagiocephaly may improve as the child grows even without active intervention.27
If the final decision is to proceed with helmet therapy, one important practical consideration prior to instituting therapy is assessing the infant’s head control. This is because the placement of a helmet for 23 hours a day would subject the infant’s head and neck to additional weight, and could potentially interfere with motor development if commenced too early. Helmet therapy should therefore only be considered after the infant is assessed to have achieved adequate head control. To this end, it is also vital to continue to be diligent with concurrent repositioning and physiotherapy exercises for the duration of helmet therapy, rather than relying merely on helmet therapy alone.
Management algorithm
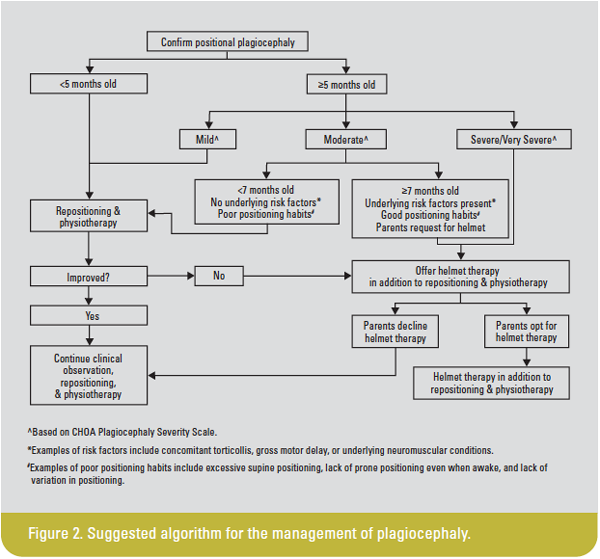
The currently accepted management of positional plagiocephaly in infants is to commence on a course of conservative therapy consisting of repositioning and physiotherapy, especially for younger infants aged ≤4 months presenting with mild-to-moderate deformity. In such cases, an improvement in cranial symmetry may be achieved with conservative therapy or observation alone. Helmet therapy should be reserved for more severe deformity, particularly in infants presenting at 5–6 months or older, or who have failed to see improvement despite conservative measures.1,32,37
Based on the current literature and taking into account the recommendations from the Congress of Neurological Surgeons Systematic Review and Evidence-Based Guidelines in 2016,1Figure 2 summarizes and illustrates a suggested algorithm for the management of plagiocephaly.
FOLLOW-UP AND OUTCOMES
The follow-up routine of infants with positional plagiocephaly should include reassessment at regular intervals to chart the progress and treatment response. Serial anthropometric measurements should be documented, and the degree of improvement may then be determined with the change in severity level. Subjective appraisals of cosmetic appearance may also be included, and parental input should be part of every reassessment. In addition to head shape, the progress of any concomitant torticollis and the infant’s development should be evaluated regularly.32
Follow-up studies have shown that in the long term, parent and child perceptions of outcomes are similar regardless of whether they chose to proceed with helmet therapy or persist with conservative management.38 By the time the children are 2–5 years of age, parents usually express little to no residual concern over their child’s head shape,27,36,38 and the long-term quality of life in children with a history of positional plagiocephaly is largely unaffected.38
CONCLUSION
Positional plagiocephaly is the most common cause of plagiocephaly and is largely benign. However, it is important to identify and exclude any underlying craniosynostosis syndrome, which can be done at a primary care level by thorough clinical assessment. Cranial measurements using a calliper should be noted as part of the assessment to calculate cranial asymmetry parameters and facilitate objective quantification. Although there is currently no standard classification system, the CHOA Plagiocephaly Severity Scale has the potential to fill this gap once it is externally validated.
Parental education on the early adoption of preventive strategies from birth is important and can decrease the likelihood of occurrence, failing which, repositioning and physiotherapy may be instituted. Helmet therapy is useful in achieving quicker improvement in head shape, but is not entirely without risk. Regular follow-up is advised regardless of choice of treatment modality. Parents should be counselled on the natural history of positional plagiocephaly and provided with reassurance as long as the child continues to achieve normal growth and developmental milestones.
About the author
Dr Pearlly Pei Qi Chang is an Associate Consultant from the Department of Paediatric Medicine at KK Women’s and Children’s Hospital, Singapore. Conflict of interest: none.