CASPIAN: Durvalumab + platinum-etoposide improves OS in ES-SCLC
05 Dec 2019
byElaine Soliven
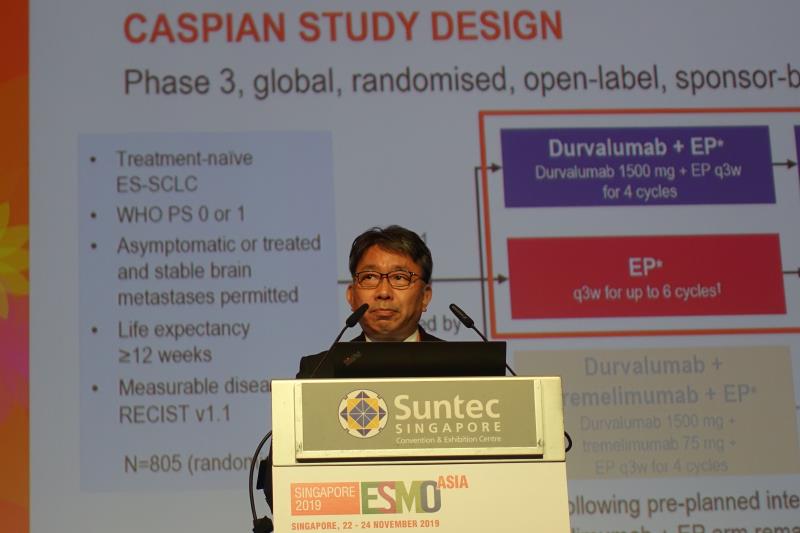 Dr Makoto Nishio
Dr Makoto NishioFirst-line treatment with durvalumab + platinum-etoposide (EP)* improves overall survival (OS) in Asian patients with extensive-stage small-cell lung cancer (ES-SCLC), according to the CASPIAN** study.
The 76 Asian patients (from Japan [n=34], South Korea [n=28], Taiwan [12], and China [n=2]) with ES-SCLC in this randomized, open-label, phase III trial were randomized to receive either durvalumab 1,500 mg + EP intravenously Q3W for four cycles and continued every 4 weeks until disease progression or EP alone intravenously Q3W for six cycles, followed by an optional prophylactic cranial irradiation as per the investigator’s discretion. [ESMO Asia 2019, abstract LBA15]
In a prespecified exploratory analysis, the OS rate at 12 months was greater among patients who received durvalumab + EP compared with those on EP alone (63.7 percent vs 49.5 percent).
Compared with EP alone, Asian patients treated with durvalumab + EP also had a higher median OS (14.8 vs 11.9 months; hazard ratio [HR], 0.87, 95 percent confidence interval [CI], 0.45–1.64), which was consistent with the global population (median, 13.0 vs 10.3 months; HR, 0.73, 95 percent CI, 0.59–0.91).
“[However], interpretation of OS in the Asia subgroup is limited due to small numbers of patients,” said Dr Makoto Nishio from the Department of Thoracic Medical Oncology at the Cancer Institute Hospital of Japanese Foundation for Cancer Research in Tokyo, Japan.
Constipation (45.7 percent vs 46.2 percent), nausea (42.9 percent vs 46.2 percent), and neutropenia (37.1 percent vs 48.7 percent) were the most common adverse events (AEs) reported in the durvalumab + EP and EP-only treatment arms.
Grade 3 or 4 AEs were more frequent in patients treated with EP alone compared with durvalumab + EP (76.9 percent vs 62.9 percent). Serious AEs occurred in 19 patients in the EP-alone arm and 15 patients in the durvalumab + EP arm. One AE event leading to death was reported in the durvalumab + EP arm.
Immune-mediated AEs of any grade occurred in 20 percent of patients, but only one patient in the durvalumab + EP arm reported a grade 3 or 4 immune-mediated AE and one patient had type 1 diabetes.
“The safety profile of durvalumab + EP in this Asian subgroup was consistent with the known safety profile of durvalumab and EP, and was generally consistent with the global population,” Nishio noted.
“Combining durvalumab with either cisplatin- or carboplatin-etoposide in ES-SCLC provides an important new treatment option for patients and physicians,” he concluded.
*EP: Etoposide 80–100 mg/m2 with either carboplatin AUC 5–6 or cisplatin 75–80 mg/m2
**CASPIAN: Durvalumab ± tremelimumab in combination with platinum-based chemotherapy in untreated extensive-stage small cell lung cancer