Clinical Applications of Anti-Müllerian Hormone as a Biomarker in Reproductive Medicine
17 Mar 2020byDr. Hang Wun Raymond Li MMedSc, FRCOG, FHKAM (O&G), Prof. Pak-Chung Ho MD, FRCOG, FHKAM (O&G), Dr. Ernest Hung Yu Ng FRCOG, FHKAM (O&G)
Dr. Hang Wun Raymond Li MMedSc, FRCOG, FHKAM (O&G)
Prof. Pak-Chung Ho MD, FRCOG, FHKAM (O&G)
Dr. Ernest Hung Yu Ng FRCOG, FHKAM (O&G)
INTRODUCTION Anti-Müllerian hormone (AMH) was initially recognized as the factor that determines regression of the Müllerian duct in the male foetus and hence plays an important role in male sex differentiation. Production of AMH in adult women was first reported in 1990.1 In the past two decades, its role in female ovarian function and the clinical utilities of serum AMH level has been increasingly studied.
ANTI-MÜLLERIAN HORMONE IN NORMAL REPRODUCTIVE PHYSIOLOGY
In the male foetus, AMH secreted by immature Sertoli cells in the testes is responsible for regression of the Müllerian duct. It is produced at relatively stable levels until puberty, and subsequently declines as testosterone increases.
In the female foetus, AMH production starts around the 36th week of gestation. Circulating AMH remains at very low levels from birth until puberty. At puberty, as ovarian folliculogenesis starts, AMH level starts to rise and peaks at around 25 years of age, after which it gradually declines with age, reaching an undetectable level around the time of menopause.2
In adult females, AMH is first produced in the ovarian follicles at the preantral stage. This gradually increases and peaks in antral follicles measuring 2–8 mm in diameter, after which AMH expression ends abruptly as the follicle enters the follicle stimulating hormone (FSH)-dependent stage.3-5
AMH plays an important role in maintaining the follicular pool and preventing it from premature depletion. Firstly, it inhibits the initial recruitment of the primordial follicles.6 Secondly, it reduces the sensitivity of the follicles to FSH, hence interfering with the cyclic recruitment.6-7
MEASUREMENT OF SERUM ANTI-MÜLLERIAN HORMONE LEVELS
Anti-Müllerian hormone assays and evolution
In the early 2000s, there were mainly two commercial manual ELISA kits for measuring AMH, manufactured by Diagnostic Systems Laboratories, Inc. (DSL) and Immunotech. These two kits were then replaced by AMH Gen II ELISA, which was marketed by Beckman Coulter, adopting the same antibodies from the DSL kit, but the calibrators from the Immunotech kit. The AMH Gen II ELISA has been the most common test kit for AMH measurements since 2010.
A previous study reported considerable within-subject variability in test results with the Gen II kit, especially upon sample dilution and storage under different conditions.8 These inaccuracies were believed to be caused by interference from complements in the serum. The manufacturer recommends a pre-mixing protocol that could deactivate the complements, hence overcoming the problem and improving assay stability under different sample storage conditions.9
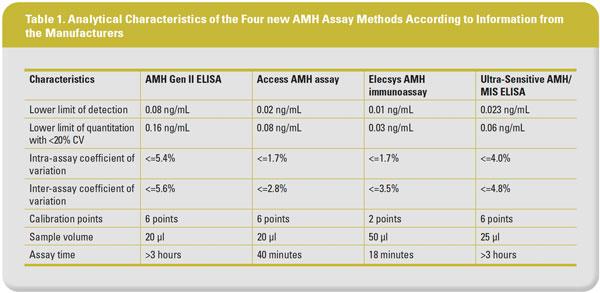
In recent years, several new AMH measurement kits have been introduced. These include the ultrasensitive AMH ELISA kit (Ansh Laboratories, Texas, USA), the automated Access AMH kit (Beckman-Coulter Diagnostics, USA), and Elecsys® AMH Immunoassay (Roche Diagnostics International Ltd, Indiana, USA). The latter two are automated immunoassays based on chemiluminescence methods. It has been shown that these two automated assays are not susceptible to interference by complements in the serum.10 Automation can theoretically minimize human errors and increase assay throughput, efficiency, and convenience. Table 1 lists the analytical characteristics of the four commercial AMH assay methods that are currently available.
Comparison between different assays
The Gen II assay showed good correlation with the older AMH ELISA kits, as well as with the newer assays including the Ultra-Sensitive AMH ELISA (Ansh Labs), Access AMH assay (Beckman-Coulter), and Elecsys AMH Immunoassay (Roche). However, these different assay methods do differ with each other in their calibration. While the Access AMH assay gives roughly equivalent values as the Gen II assay, the values given by the Elecsys AMH Immunoassay (Roche) and the Ultra-Sensitive AMH ELISA (Ansh Labs) are 0.88-fold and 1.77-fold of the Gen II assay.11 The AMH values generated by all the three newer assay methods were significantly altered after freezing and thawing of serum samples, but the magnitudes of change were very small and perhaps not clinically important for the two automated platforms. All the three new assay methods had good intra- and inter-assay precision.11 An international standard is urgently needed before widespread clinical use of AMH assays can be properly developed. Adapting clinical cut-offs by direct conversion from previous studies that used different assay methods is not recommended. Instead, it may be more appropriate to redefine these cut-off values by further clinical studies when a unified international standard is available.
Intra- and inter-cycle variations of serum anti-Müllerian hormone levels
Most studies have demonstrated that there are small fluctuations in serum AMH levels within and between menstrual cycles. A number of studies have reported a mild decline of serum AMH levels in the late follicular phase as AMH expression ceases in the dominant follicle; some revealed that intra-cycle variation was higher in women with high AMH levels than those with low AMH levels. However, the magnitude of the fluctuations is generally small and may not be clinically important.12 A previous study revealed that the intra-cycle fluctuations were within the same quintile in 72% of women and crossed two quintiles in only 1%.12 Two prospective studies12-13 suggested that only 11% of the inter-cycle variability resulted from intra-individual fluctuations between cycles (intra-class coefficient 0.89). This means that AMH can be measured on any day of the menstrual cycle.
Other external factors into play
There was a negative correlation between body mass index (BMI) and serum AMH level in a meta-analysis that included 45 published studies of fertile and infertile women.14 It is postulated that obesity may exert apoptotic effect on ovarian granulosa cells. However, the exact mechanisms that mediate the reduction in AMH production in obesity remain uncertain. The effects of combined oral contraceptives15 and cigarette smoking16-17 on serum AMH are more controversial, with conflicting results reported in the literature.
Age-specific reference ranges of serum anti-Müllerian hormone in women
Since the serum AMH concentration changes with women’s age, age-specific reference ranges based on large populations need to be established to put the assay results into clinical utility. As there is currently no international standard for AMH measurement, and the numerical values generated by different existing assay methods differ, assay-specific reference ranges are needed to put each individual assay methods into clinical context. Moreover, interethnic variations in serum AMH concentrations have been demonstrated, with lower values observed among African-American and Hispanic women than among Caucasians.18-19 Therefore, individual reference ranges need to be established for specific ethnicities as well.
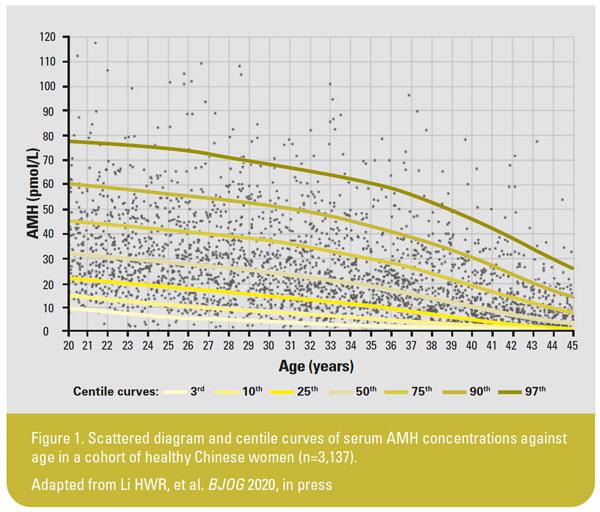
While there have been a few published age-specific reference ranges in large population studies using the manual AMH ELISA methods, only a few has been available for the new automated assays. Some of these references ranges were established in women consulting for infertility, which may constitute a biased group as some of these women might have abnormal AMH levels secondary to underlying anovulatory disorders. There was one set of age-specific reference ranges recently published for the automated AMH assay by Beckman-Coulter in the Chinese population,20 where the subjects were stratified by five-yearly age groups. A set of age-specific reference ranges in a larger healthy cohort of the Chinese population stratified by one-yearly age groups was recently published (Figure 1).
CORRELATION OF SERUM ANTI-MÜLLERIAN HORMONE LEVEL AND OVARIAN RESERVE
The primordial follicle count is considered the parameter representing the ovarian reserve in a woman, but it is not practically measurable in the clinical setting. Hence, surrogate markers that correlate closely with the primordial follicle count have been explored for clinical use, and both the AMH level measured from the serum and the antral follicle count (AFC) measured sonographically have been proven to serve this purpose.
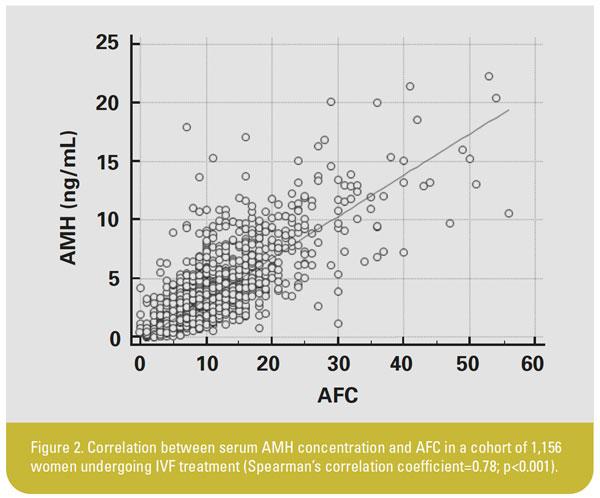
A previous study on 42 women undergoing oophorectomy for benign gynaecological conditions revealed significant correlations (correlation coefficient 0.72; p<0.0001) between serum AMH level and the ovarian primordial follicle count determined histologically.21 Most studies showed significant and high correlation between serum AMH level and AFC. Data from a cohort of 1,156 women from Hong Kong revealed a Spearman correlation coefficient of 0.78 (p<0.001) between AMH and AFC (Figure 2).
Anti-Müllerian hormone as a biomarker in assisted reproduction
Ovarian stimulation and intrauterine insemination
A retrospective study in Hong Kong22 first reported that women undergoing ovarian stimulation and intrauterine insemination (IUI) who attained live birth either during the first treatment cycle or cumulatively over three treatment cycles had significantly higher serum AMH levels compared with those who did not. The area under the receiver-operator characteristic (ROC) curve of serum AMH in predicting first-cycle and cumulative live birth rates were 0.682 and 0.668, respectively, which indicated only modest predictive values, although it was better than that of AFC and serum FSH concentrations. Similar results have been reported in later studies.
In vitro fertilization
In many in vitro fertilization (IVF) units, ovarian reserve markers are commonly used to predict ovarian responses. Among the markers studied for this purpose, AMH and AFC are the best predictors of both poor and excessive ovarian responses.23-24 In two individual patient data meta-analyses23-24 studying prediction of excessive and poor ovarian responses, both AMH and AFC had similar and reasonably good performance in predicting ovarian response. The area under the ROC curve for AMH and AFC in predicting excessive response were 0.81 and 0.79, respectively. Combining AMH and AFC demonstrated an AUC of 0.85, and further adding age or FSH did not improve the prediction. The area under the ROC curve for AMH and AFC in predicting poor response were 0.78 and 0.76, respectively, and combining both, or adding age, did not significantly improve the prediction.
However, both AMH and AFC were poor predictors of pregnancy or live birth in the fresh IVF cycle.25-26 A meta-analysis26 of 13 studies showed an area under the ROC curve of 0.61 (95% confidence interval [CI], 0.56–0.65) of predicting live birth after IVF by AMH, indicating its poor predictive accuracy.
Apart from looking at the pregnancy or live birth rates in the fresh IVF cycle, it is also important to look at the predictive performance of AMH on cumulative pregnancy or live birth rates from fresh and all frozen-thawed embryo transfer cycles combined. This is because embryo cryopreservation has become an integral part in IVF programmes, and “freezing all” has been practiced much more frequently for various reasons. This was first reported in a retrospective cohort study of 1,156 women in Hong Kong,27 and revealed that those who achieved cumulative live birth had a significantly higher serum AMH at baseline before ovarian stimulation. However, the predictive performance of serum AMH on the absolute occurrence of cumulative live birth was only modest (area under the ROC curve was 0.65) and did not add significant value on top of the women’s age.
One major role of AMH measurement in an IVF programme is to guide the starting dose of gonadotrophin in ovarian stimulation, based on its good predictive performance on ovarian response similar to AFC. Two randomized controlled trials on women undergoing IVF, using the GnRH agonist and antagonist protocols respectively, suggested that the proportion of cycles attaining desired response was not different when the gonadotrophin dosing algorithm was determined based on either AMH or AFC.28-29
Discordance between the AMH and AFC occurs in some women undergoing IVF. Based on a retrospective cohort of women in Hong Kong, when the AMH and AFC categories are discordant, those with a higher AMH within the same AFC quartile had significantly more oocytes retrieved and higher cumulative live birth rate, and the ovarian responsiveness was intermediate between those where both were concordant on either end.30 Hence, both AMH- and AFC-based algorithms for gonadotrophin dosing can be recommended. When the AMH and AFC fall into discordant categories, it is reasonable to adopt an intermediate dose of gonadotrophin than those with concordant AMH and AFC categories on either end. Such recommendation would need to be confirmed in future prospective clinical trials. Furthermore, it has recently been shown that the ovarian response prediction index (ORPI), calculated as the serum AMH (ng/mL) multiplied by the AFC and divided by the age of the woman (years) is superior to the individual components alone in predicting ovarian response.31
Clinical utility of anti-Müllerian hormone in reproductive endocrinology
Differential diagnosis of disorders of sex development
In pre-pubertal boys, as AMH is mainly produced from Sertoli cells, its level in the blood serves as a useful marker to distinguish between cryptorchidism and anorchia in boys without palpable testis. A normal AMH level would indicate the presence of testis. Serum measurement of AMH together with testosterone levels also helps to differentiate disorders of sexual development due to gonadal dysgenesis from those due to defective androgen production or action. Low AMH and low testosterone levels is suggestive of testicular dysgenesis; normal AMH and low testosterone levels is indicative of Leydig cell-specific disorders, while low AMH and normal testosterone level may result from AMH gene mutations. Disorders of sexual development with normal levels of both AMH and testosterone may result from androgen target organ defects (eg, androgen insensitivity syndrome, 5-alpha reductase deficiency or AMH receptor defect) or other structural malformations.32
Differential diagnosis of anovulatory disorders
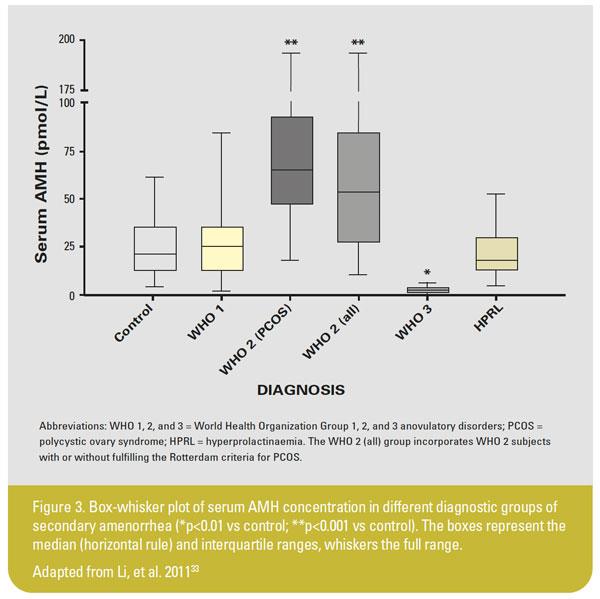
The main causes of anovulatory disorders, commonly presented as oligomenorrhoea or amenorrhea, include: (1) hypogonadotropic hypogonadism; (2) normogonadotropic normogonadic anovulation (predominantly due to PCOS); (3) hypergonadotropic hypogonadism (premature ovarian insufficiency, POI); and (4) hyperprolactinemia. Measuring the hormonal profile including serum FSH, LH, oestradiol, and prolactin levels helps in distinguishing these conditions.
It has been shown that serum AMH level is significantly higher in patients with normogonadotropic anovulation, both with or without PCOS, and is reduced to very low or undetectable levels in patients with POI, but is unchanged in patients with hypogonadotropic hypogonadism and hyperprolactinaemia, compared with normal ovulatory controls, as illustrated in Figure 3.33
A meta-analysis34 of studies on the use of serum AMH levels in diagnosing PCOS showed that a cut-off value of AMH at 4.7 ng/mL had an overall sensitivity of 82.8% and specificity of 79.4% in diagnosing PCOS in symptomatic women, and the area under the summary ROC curve based on aggregated individual patient data was 0.87 (95% CI, 0.83–0.92). Nonetheless, various diagnostic cut-off values of AMH ranging from 4.2–8.4 ng/mL were proposed for discriminating women with PCOS from normal controls among the different studies included in the review. This could be attributed to the different assay methods used with different calibration and age-related changes in the serum AMH concentration. Hence, AMH is not considered to be a diagnostic criterion for PCOS at the moment.35
Prediction of natural menopause
As a surrogate marker of ovarian reserve, AMH has been studied for its role in predicting the timing of natural menopause. Theoretically, such prediction may allow the woman to estimate her remaining reproductive lifespan, facilitating one’s family and fertility planning. Some studies showed that serum AMH level declined to undetectable levels around 3–5 years before menopause.36-37 A recent prospective study also showed that serum AMH levels were significantly lower in women with early menopause before the age of 45 after adjusting for BMI, smoking, parity, oral contraceptive use, history of infertility, and menstrual cycle characteristics.38
There have been a few studies which showed that women with lower age-specific AMH levels would experience menopause earlier than those with higher age-specific AMH levels; yet the confidence intervals of the predicted age at menopause is very wide in all these studies, spanning up to over 10 years, meaning that the prediction lacks precision.39-41
Management of cancer survivors
Serum AMH measurement has also been studied for prediction of ovarian damage after gonadotoxic cancer treatments. A prospective study of women with newly diagnosed breast cancer revealed that those who continued to menstruate at 5 years post-chemotherapy had a significantly increased pre-treatment serum AMH.42 A predictive tool for ongoing ovarian function after chemotherapy or radiotherapy has been developed incorporating serum AMH and age of the woman as the parameters.43 This may allow individualized advice to be given regarding fertility preservation measures prior to commencing cancer treatment.44 Nonetheless, most of the current studies reported only on menstrual outcome or ovarian function parameters, and there is little data regarding the long-term fertility outcome in cancer survivors.
Measuring post-treatment serum AMH levels may also aid decision on adjuvant treatments. Undetectable serum AMH 2 years following gonadotoxic treatment may indicate extremely low likelihood for resumption of ovarian function.45 These patients may be considered for adjuvant treatment regimens that are suitable for post-menopausal status, for instance aromatase inhibitors in survivors of hormone-sensitive breast cancer.44
ANTI-MÜLLERIAN HORMONE IN FERTILITY PREDICTION
Contrary to common belief, evidence suggests a limited role for AMH in predicting natural fecundability in the general population. A few prospective cohorts revealed no significant difference in serum AMH level between women who got pregnant within 6–12 months and those who did not.45-48 Overall, the use of serum AMH as a basis of fertility counselling is not supported by good evidence. The finding suggests that decreased ovarian reserve may result in unnecessary anxiety, and that “normal” ovarian reserve may confer false reassurance which may unduly delay fertility planning. Many women may consider advancing their fertility planning at the expense of other life goals if being told of a reduced ovarian reserve, and some may consider preventive oocyte cryopreservation, and yet the clinical cut-off to prompt such actions is currently uncertain.
CONCLUSION
AMH is a useful tool in assessing ovarian reserve in adult female. It is strongly correlated with both the primordial follicle pool (the ovarian reserve) and AFC (the active follicular pool). Compared with AFC, the measurement of AMH is less operator-dependent and can be performed randomly on any day of the menstrual cycle. AMH measurement in women is being investigated for a number of clinical applications including prediction of ovarian response in assisted reproduction treatments and differential diagnosis and management of anovulatory disorders. However, there have been different newer assay methods for serum AMH, and their comparability, reference ranges, and clinical cut-offs need to be evaluated further.
About the authors
Dr Hang Wun Raymond Li is a Clinical Associate Professor from the Department of Obstetrics & Gynaecology, The University of Hong Kong, Queen Mary Hospital, Hong Kong. Conflict of interest: none.
Professor Pak-Chung Ho is an Emeritus Professor from the Department of Obstetrics & Gynaecology, The University of Hong Kong, Hong Kong. Conflict of interest: none.
Dr Ernest Hung Yu Ng is a Clinical Professor from the Department of Obstetrics & Gynaecology, The University of Hong Kong, Queen Mary Hospital, Hong Kong. Conflict of interest: none.