MYSTIC: Durvalumab ± tremelimumab vs chemotherapy may benefit Asian patients with metastatic NSCLC
09 Dec 2019
byElaine Soliven
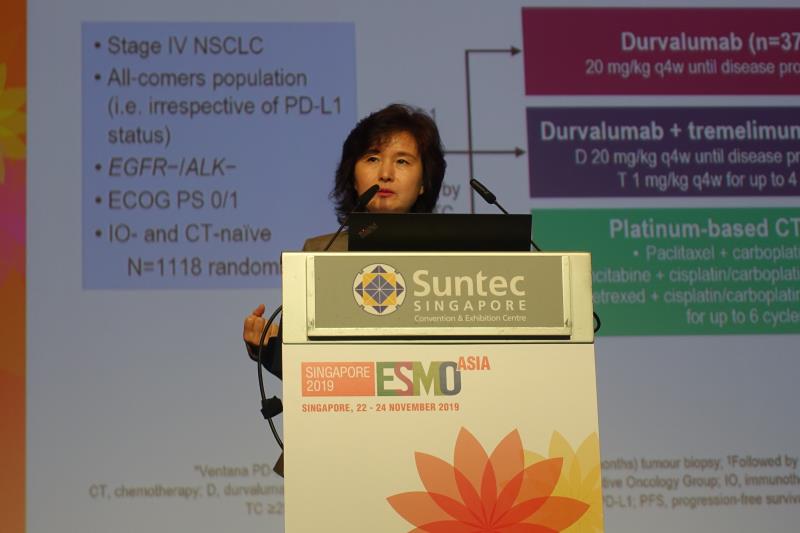 Dr Myung-Ju Ahn
Dr Myung-Ju AhnTreatment with durvalumab with or without tremelimumab appeared to improve overall survival (OS) in Asian patients with metastatic non-small cell lung cancer (mNSCLC) compared with chemotherapy (CT) in the first-line setting, according to a post hoc analysis of the MYSTIC* trial presented at ESMO Asia 2019.
This multicentre, open-label, phase III trial involved 488 patients with mNSCLC who had PD-L1 tumour cell (TC) expression of ≥25 percent. Participants were randomly assigned to receive durvalumab** alone (n=163 overall [59 Asians]), durvalumab** + tremelimumab 1 mg/kg every 4 weeks for up to four doses (D+T group; n=163 overall [50 Asians]), or platinum-based CT*** (n=162 overall [47 Asians]) for up to six cycles. The primary analysis has been reported in the 2018 ESMO Congress. The current post hoc analysis was on 156 Asian patients, which made up 32 percent of the overall intent-to-treat population. [ESMO Asia 2019, abstract 474O]
In this subgroup analysis of Asian patients, an improved median OS was observed among those who received durvalumab alone compared with CT (18.8 vs 10.6 months; hazard ratio [HR], 0.69, 95 percent confidence interval [CI], 0.43–1.09), although the difference was not statistically significant. These OS results were consistent with the overall population (16.3 vs 12.9 months; HR, 0.76, 95 percent CI, 0.56–1.02).
An improved median OS was also observed among Asian patients treated with D+T than those who received CT (17.7 vs 10.6 months; HR, 0.64, 95 percent CI, 0.40–1.03), “but the number is quite small, so we should be very cautious in interpreting these data,” said Dr Myung-Ju Ahn from Samsung Medical Center in Seoul, South Korea.
Consistent with the overall population, median progression-free survival (PFS) was found to be slightly longer in the D+T arm than the CT arm (5.5 vs 4.2 months; HR, 0.79, 95 percent CI, 0.49–1.28), while PFS was comparable between the durvalumab alone and CT arms (4.1 vs 4.2 months; HR, 0.84, 95 percent CI, 0.53–1.36).
All treatment arms showed similar overall response rates at 32.2 percent, 36.0 percent, and 36.2 percent, which were also consistent with the overall population at 35.6 percent, 34.4 percent, and 37.7 percent (for durvalumab alone, D+T, and CT, respectively).
However, the rate of subsequent anticancer therapy was higher among Asian patients compared with the overall population in the D+T arm (60.0 percent vs 37.4 percent ).
“[Nevertheless,] exploratory OS and PFS analyses in patients with PD-L1 TC ≥25 percent in the Asian group showed favourable HRs for durvalumab monotherapy and D+T vs CT,” Ahn noted.
“In MYSTIC [trial], while statistical significance was not achieved, a clinically meaningful improvement in OS was observed for first-line durvalumab vs CT in patients with mNSCLC and PD-L1 TC ≥25 percent,” Ahn concluded.
Grade 3 or 4 treatment-related adverse events (AEs) occurred more frequently in the D+T arm than the durvalumab alone arm (23.9 percent vs 19.7 percent), which was expected and manageable, Ahn noted.
The D+T arm also had a higher rate of serious AEs than the durvalumab alone and CT arms (25.6 percent vs 11.5 percent and 7.2 percent), which leads to treatment discontinuation at 9.0 percent, 14.5 percent, and 7.2 percent in the durvalumab alone, D+T, and CT treatment arms, respectively.
“The safety profile of durvalumab ± tremelimumab in the Asian subgroup was manageable and consistent with the overall MYSTIC population and previous studies,” Ahn noted.
*MYSTIC: Phase III open-label first-line therapy study of MEDI 4736 (durvalumab) with or without tremelimumab versus SOC in non-small cell lung cancer (NSCLC)
**Durvalumab: Dosage at 20 mg/kg every 4 weeks and continued until disease progression
***Platinum-based chemotherapy: Paclitaxel + carboplatin, gemcitabine + cisplatin/carboplatin for squamous cell or pemetrexed + cisplatin/carboplatin for non-squamous cell