INTRODUCTION
Hypoglycaemia is one of the most common clinical issues facing newborn babies. It can be caused by abnormalities in the glycogen stores, alternative substrates, and/or functioning enzymes. The definition of neonatal hypoglycaemia itself remains challenging. Understanding normal glucose physiology and biochemistry is important so that the neonatologist can initiate appropriate investigations to elucidate an aetiology and institute correct management. Early diagnosis and prompt treatment of hypoglycaemia will reduce the risk of brain injury to the developing child.
The foetus depends on a continuous placental supply of glucose and other substrates for energy, including ketones, free fatty acids, and amino acids for metabolic demands and energy needs in utero. At birth, the umbilical cord is clamped thus leading to an abrupt cessation of the exogenous glucose supply from the mother, which results in a fall of neonatal blood glucose concentrations over the ensuing 4–6 hours, reaching a nadir of about 2.5 mmol/L.1
The homeostatic response is a decrease in insulin secretion, coupled with a surge in counter-regulatory hormones including glucocorticoids, catecholamines, and glucagon. This is dependent on an effective and functioning glycogenolysis system with adequate stores of glycogen, and intact gluconeogenesis, which utilizes alternative substrates of amino acids, lactate, and glycerol. Hence, apart from stabilization of blood glucose levels, the neonate adapts and copes with a relative state of hypoglycaemia due to initial lower blood sugar levels. During this period, the neonate is usually asymptomatic, while the glycaemic supply is switched from a constant infusion via the placenta to an enteral form with established feeding. Blood sugar levels then rise and stabilize after 48–72 hours of life.2
While neonatologists rely on a working definition of neonatal hypoglycaemia based on a numerical value for pragmatic reasons, the true definition is the concentration of glucose in the blood or plasma at which the individual demonstrates a unique response to the abnormal milieu caused by the inadequate delivery of glucose to a target organ.3 Symptomatic hypoglycaemia occurs where there are inadequate compensatory mechanisms via gluconeogenesis and glycogenolysis, as well as insufficient alternative supply of substrate for oxidative metabolic functions.4 This adaptive response is also compromised if there is persistent hyperinsulinemia, as this limits the production of alternative substrates. This can happen due to incomplete suppression of insulin secretion secondary to immaturity of the pancreatic β-cell.5
Inadequate energy supply, whether through glucose or otherwise, causes adrenergic or neurogenic and neuroglycopenic symptoms. Adrenergic symptoms result from the activation of the sympathetic nervous system, manifesting in sweating, pallor, irritability, hunger, vomiting, and tremulousness. Objective non-specific signs include tachycardia and hypothermia. Neuroglycopenia symptoms signify decompensation, with hypotonia, seizures, altered consciousness with either lethargy or encephalopathy resulting in high-pitched cry, or poor suck/feeding. Neurological injury can be seen radiologically, producing the classic parieto-occipital pattern predominance of abnormally high white matter signal intensities and even loss of grey-white matter differentiation. Furthermore, widespread neurological injury can be seen in other regions of the brain as well, from basal ganglia, thalamic, cerebellar lesions, to widespread cortical changes.6
NEONATES AT-RISK OF HYPOGLYCAEMIA
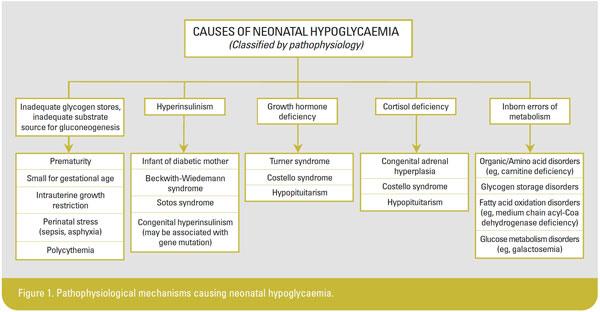
There is a range of “profiles” that puts a neonate at increased risk of developing non-physiological hypoglycaemia, with a defective adaptive response. Low sugar levels are most common among infants born prematurely or small-for-gestational-age due to insufficient glycogen stores in the liver and limited ability to utilize alternative substrates. Babies born to mothers with poorly controlled insulin-dependent diabetes mellitus may develop hypoglycaemia secondary to the presence of circulating insulin released by the foetal pancreas in response to high sugar levels transferred via the placenta. Less common reasons for low sugar levels in babies include the inborn errors of metabolism, endocrine (growth hormone and cortisol) deficiencies, and pathological hyperinsulinemic state, as well as inadequate glycogen stores and alternative substrate supply5 (see Figure 1). Neonates with transient and physiological hypoglycaemia usually improve by 48–72 hours of life.
Neonates with persistent hypoglycaemia must be duly evaluated because such patients commonly require prolonged intravenous infusions of fluids with high glucose infusion rates (GIRs). Withholding investigation leads to delay in both diagnosis of underlying metabolic/endocrine conditions and administration of effective treatment. The definition of persistent hypoglycaemia varies from institution to institution, ranging from hypoglycaemia that lasts for >48 hours up to 7 days of life.7-8 Non-physiological causes of hypoglycaemia should also be considered if high GIRs are persistently required, with the lower limits of GIR ranging from 8–12 mg/kg/minute.8-9 Challenges in investigating neonates with persistent hypoglycaemia include the need to take critical samples in the midst of hypoglycaemia. In the absence of hypoglycaemia, a provocative fasting test or controlled reduction of GIR should be performed to obtain the required specimens for diagnosis.7 The suggested work-up to delineate the aetiology of persistent hypoglycaemia includes serum insulin, glucose, ketones, free fatty acids, cortisol, and growth hormone levels.
CONTROVERSIES AND KNOWLEDGE GAPS
Neonatal hypoglycaemia worries doctors and parents alike because of its possible adverse long-term neurodevelopmental effects. Lucas, et al, demonstrated in a multicentre study involving 661 preterm infants that the degree and duration of hypoglycaemia directly correlated with poorer Bayley’s motor and mental developmental scores at 18 months.10 Although disparities in certain developmental domains improved by 5 years of age in comparison with their normoglycaemic counterparts, deficiencies and impairments remained in arithmetic, language, and motor tests.11 The fasting plasma glucose threshold was found to be most significant at 2.6 mmol/L. Thereafter, most neonatal units use 2.6 mmol/L as an operational threshold, and treatment is administered to correct “hypoglycaemia” when this is met. Multiple studies have subsequently demonstrated similar associations12-13 between blood glucose levels of <2.6 mmol/L and impaired developmental outcomes. It is important however to consider that in many studies, sample patients were preterm neonates who themselves have impaired metabolic adaptive mechanisms and limited functional capacity to regulate glycaemic control, as well as baseline prior neuronal maldevelopment. The effects have not been conclusively seen in term infants. Furthermore, studies with robust methodologies demonstrated that a threshold of blood sugar level lower than 2.6 mmol/L made no difference to neurodevelopmental outcomes, both short and long term. Win, et al, conducted a prospective observational trial of preterm infants born at <32 weeks’ gestational age with long follow-up periods of up to 15 years, where no significant differences in neurocognition were found between patients with hypoglycaemia and matched controls.14 In a prospective cohort study, McKinlay, et al, studied 528 neonates born at >35 weeks’ gestation using continuous interstitial glucose concentrations that were masked to clinical staff. No association was found between hypoglycaemia and neurosensory impairment or cognitive processing difficulties at 2 years of age.15
Despite the absence of neurocognitive differences between normal and hypoglycaemic newborns in several cohort studies, the National Health Service Litigation Authority reported over £162,166,677 in damages paid between 2002 and 2011 to neonatal hypoglycaemic patients who had suffered long-term deleterious neurodevelopmental outcomes.16 There is hope though, with main gaps identified being “failure to assess risk factors and commence glucose monitoring”, “failure to recognize clinical signs and history”, and “delay in acting upon abnormal blood glucose result”. Risk stratification showed that four categories of newborn babies are at increased risk for long-term neurocognitive impairment due to hypoglycaemia, including (i) babies with more profound hypoglycaemia, (ii) babies with a longer duration of hypoglycaemia, (iii) babies with clinical signs, and (iv) babies belonging to an underlying at-risk group (infant of diabetic mother, preterm, small-for-gestational-age, or inborn errors of metabolism).17 Hence, as long as a unit monitors glucose levels in at-risk groups (such as those in Figure 1), examines carefully for signs and symptoms of hypoglycaemia, and follows up with swift and decisive administration of hypoglycaemia treatment when required, there is a possibility that lower thresholds may be adopted in future.
CURRENT SOCIETAL GUIDELINES
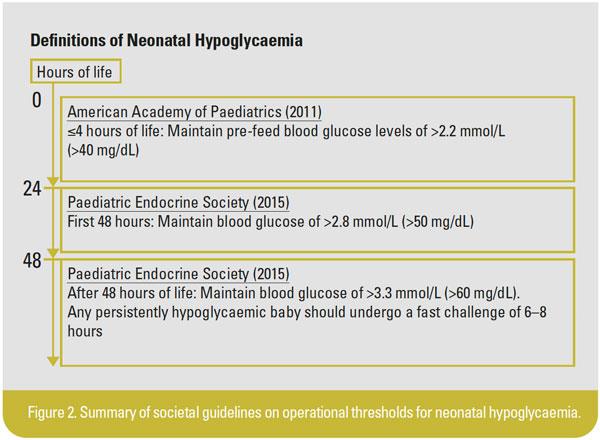
The American Academy of Paediatrics18 (AAP, 2011) and Paediatric Endocrine Society7 (PES, 2015) have developed guidelines on the approach to neonatal hypoglycaemia (Figure 2). Taking into account the transient physiologic nature of neonatal hypoglycaemia, both routine screening and monitoring of blood glucose are not indicated in healthy term infants after an otherwise normal pregnancy and delivery. With the pathophysiological “risk profile”, screening is recommended for neonates who have impaired adaptive transitional physiology and are at risk of impaired glucose homeostasis, namely, those who are small-/large-for-gestational-age, infants of diabetic mothers, preterm infants, or those with clinical manifestations of symptomatic hypoglycaemia. The AAP recommends maintaining a blood glucose level of 2.5 mmol/L or higher during the first 24 hours of life, while the PES recommends maintaining blood glucose levels of >2.8 and 3.3 mmol/L for ≤48 and >48 hours of life, respectively.
MANAGEMENT OF NEONATAL HYPOGLYCAEMIA
In addition to the need to improve blood glucose concentrations, the attending clinician should ensure minimal disruption of rooming-in with the baby’s own mother, so that the mother can practise skin-to-skin care and promote mother-child bonding for its long-term beneficial effects. Hence, as best as possible, enteral feeding should be encouraged as a modality of managing hypoglycaemia, concomitant with an increase in daily fluid volume administered. It is well known that breastfeeding has clear benefits for the newborn baby and breast milk contains higher ketone levels19 that offer neuroprotection. Nevertheless, direct latch-on for breastfeeding has its inherent difficulties in objectively quantifying volume, predictability and adequacy of volume, and requires the baby to have “pre-feed alertness”, a sign that may not be present in symptomatic babies. In mothers who experience difficulty in establishing a steady supply of breast milk and turn to formula milk as a convenient instant solution, it must be noted that formula milk disrupts initiation/establishment of breastfeeding, and alters the innate intestinal microbiome, which has been associated with necrotizing enterocolitis in preterm infants and increases the risk of developing atopy later on in life.
Oral dextrose gel (200 mg/kg) applied to the neonate’s buccal mucosa before feeding has been shown to be effective in improving blood glucose concentrations19 within the first 48 hours after birth. It has also been shown to improve breastfeeding outcomes and maintain a gentler trend of blood sugar levels without post-treatment hyperglycaemia or rebound hypoglycaemia. Ter, et al,20 reported the efficacy and safety of dextrose gel in correcting hypoglycaemia and reducing Neonatal Intensive Care Unit (NICU) transfers, thereby minimizing separation of the baby from the mother. In another study, similar neurodevelopmental and cognitive outcomes were observed at 2 years of age among children who were treated with either oral dextrose gel or parenteral fluids.21 Despite these encouraging short-term results, there were concerns regarding the potential adverse long-term neurodevelopmental effects of dextrose gels due to potential delays in definitive treatment with intravenous dextrose, rapid overcorrection and iatrogenic hyperglycaemia, and increase in variability of glucose concentrations. Of note, these studies were undertaken in centres with very high rates of aggressive breastfeeding. While the use of oral dextrose gel is promising, it should only be performed in centres where doctors are able to have a close follow-up of subsequent glucose concentrations, monitor for clinical signs of hypoglycaemia, and document its resolution.
Parenteral treatment must be provided in preterm infants for whom feeding is contraindicated (ie, concerns of necrotizing enterocolitis), feeding intolerance is an issue, or enteral options are unsuccessful. An intravenous bolus of dextrose 10% (200 mg/kg or 2 mL/kg) must be administered followed by maintenance fluids with a GIR of at least 8 mg/kg/minute.19 This has been shown to restore normoglycaemia rapidly within 1 minute.22
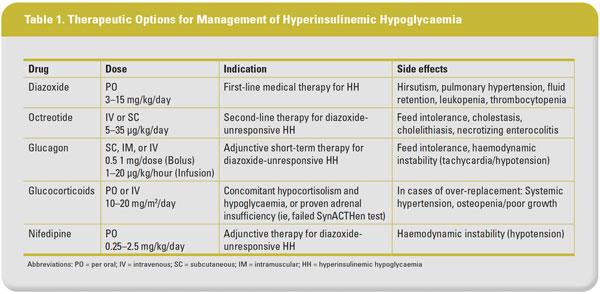
Additional medical/surgical modalities of treatment23 (refer to Table 1) may be considered when there is failure to wean high GIR levels. These include reducing insulin secretion with utilizing diazoxide or octreotide, stimulating hepatic glycogenolysis and catecholamine release to counter-regulate. However, recent studies have reported adverse effects of diazoxide treatment in babies with persistent hypoglycaemia, including fluid overload with resultant heart failure and necrotizing enterocolitis.24-25 Glucagon can be administered as a short-term measure, but rebound hypoglycaemia does occur with glucagon use. Rarely, clinicians may need to resort to using nifedipine (a calcium-channel blocker), glucocorticoids, or pancreatic surgery. Whilst pancreatectomy removes the source of insulin over-production, it is often associated with risks of developing exocrine and endocrine insufficiency.
While attempting to normalize glucose levels, it is important to note that swings in glucose levels are equally deleterious. High glucose variability is strongly associated with neuronal injury and mortality, which is postulated to be related to the development of reactive oxygen species and cerebral perfusion changes15 similar to the reperfusion injury mechanism.
CONCLUSION
There is now a better understanding of neonatal hypoglycaemia and transitional physiology that occurs within the first few hours to days of life of the newly born. Prospective, multicentre cohort studies are evaluating the safety of lowering operational thresholds for hypoglycaemia and developing point-of-care or rapid turnover tests to evaluate alternative metabolic substrates such as ketones/fatty acids. Current practices are based on numerical values of blood glucose levels. The long turnaround time to obtain results of blood ketone or fatty acid levels indicates that these assays have limited impact in clinical practice. Appreciating normal glucose physiology and biochemistry is important so that with early diagnosis, close monitoring, and prompt treatment of neonatal hypoglycaemia, our newly born patients will have the best chance to achieve a normal neurodevelopment.
About the authors
Dr Daniel Chan is a Senior Resident in the Department of Paediatric Medicine at KK Women’s and Children’s Hospital, Singapore. Conflict of interest: none.
Clinical Associate Professor Daisy Kwai-Lin Chan is Senior Consultant in the Department of Neonatal & Developmental Medicine, Singapore General Hospital, Singapore. Conflict of interest: none.